Combinatorial Failure Modes of Suture Anchors in Osteoporotic Bone
Team: Zachary Astle, Britney Dikwa-Nkrumah, Cameron Miller, Ezra Johnson
Sponsor: Wellstar Health
I. Abstract
Goal : Analyze the biomechanical properties of high tensile suture anchors in osteoporotic bone, which will effectively reduce arthroscopic joint repair failure, increase the strength of the joint repair, and boost patient satisfaction.
Approach : Designed an Instron testing apparatus that allows for cyclical tensile loading of the anchor inserted into osteoporotic polyurethane bone blocks which model the human shoulder
Results : Suture elasticity cannot be ignored when analyzing rotator cuff repair failure. Suture anchors should be inserted at an angle relative to the plane of the bone face that is greater than 90 degrees to avoid failure of the bone or the anchor.
II. Introduction
Due to the exponential growth of the human population and unprecedented increased life expectancy, society will have a greater number of elderly people than ever before in the coming years. Within the US, the number of adults over 65 is expected to increase from 46 million to 90 million by 2050 [4]. In the United States, an estimated 75,000 rotator cuff surgeries are performed annually, and this number is likely to rise given an aging population [5].
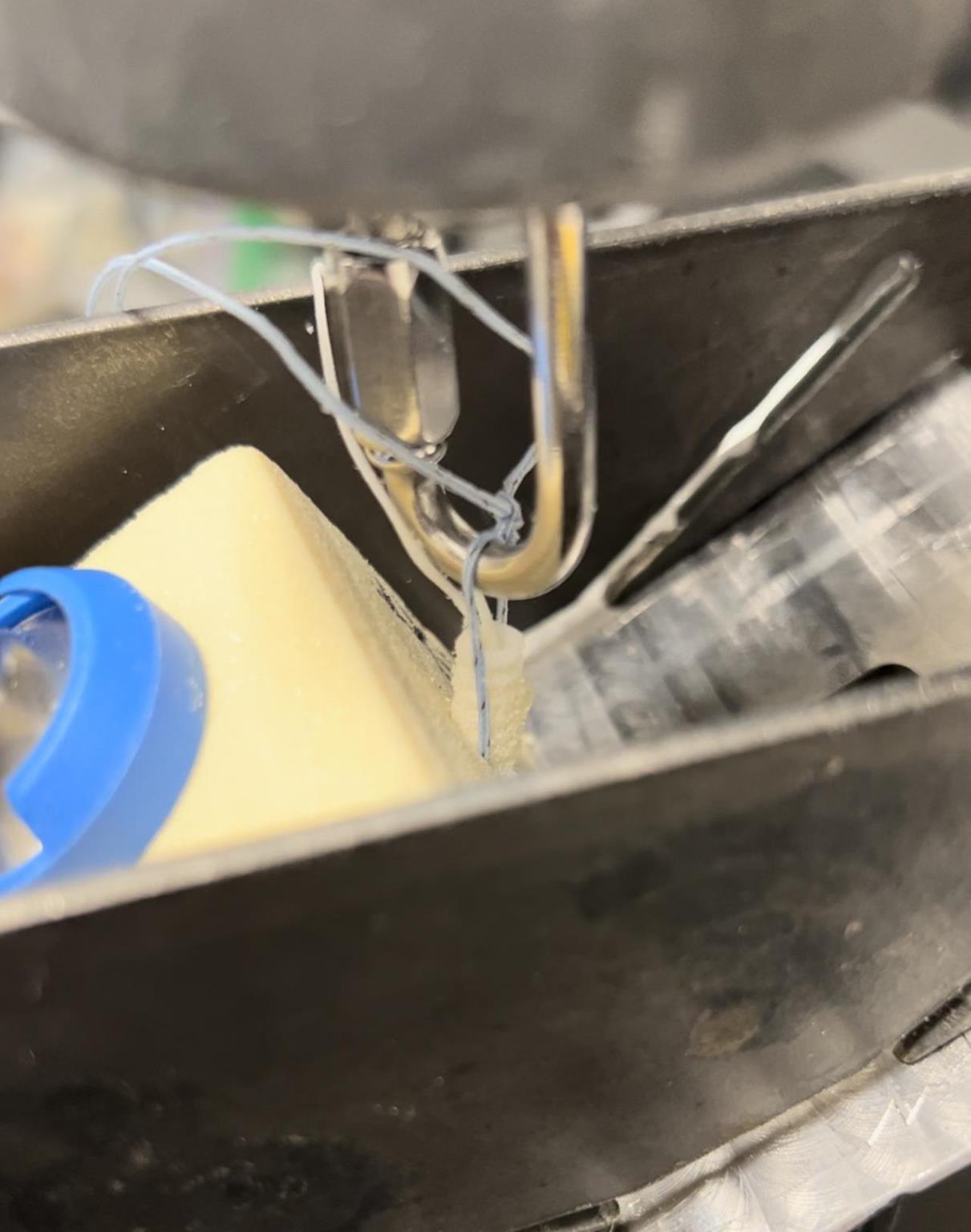
Figure 1: Suture Anchor Repair Failure
There is a need to quantify and experimentally determine the optimum angle of suture anchor insertion to halt bone sawing. Suture anchors are already highly developed and although there is always a need for innovation of new anchor designs, there is a greater need to determine the optimum insertion environment and specifications for the suture anchors on the current market, especially within osteoporotic bone. This system optimization includes discovering the optimal angle of insertion as well as loop diameter, knot location, and type of anchor (internal or external suture).
III. Methods
An Instron tensile testing apparatus was used to simulate the tensile, cyclical loading of the human shoulder. Both external suture anchors and internal suture anchors were tested at insertion angles of 30, 45, 60, and 120 degrees as shown in the figure below. The pull angle was 30 degrees to the surface of the bone to replicate human shoulder anatomy. Low density PCF bone block was used as a substitute for cadaveric samples.

Figure 2: Diagram of Insertion Angles for Both Internal and External Anchors

Figure 3: External (top) vs Internal (bottom) Anchor
IV. Results
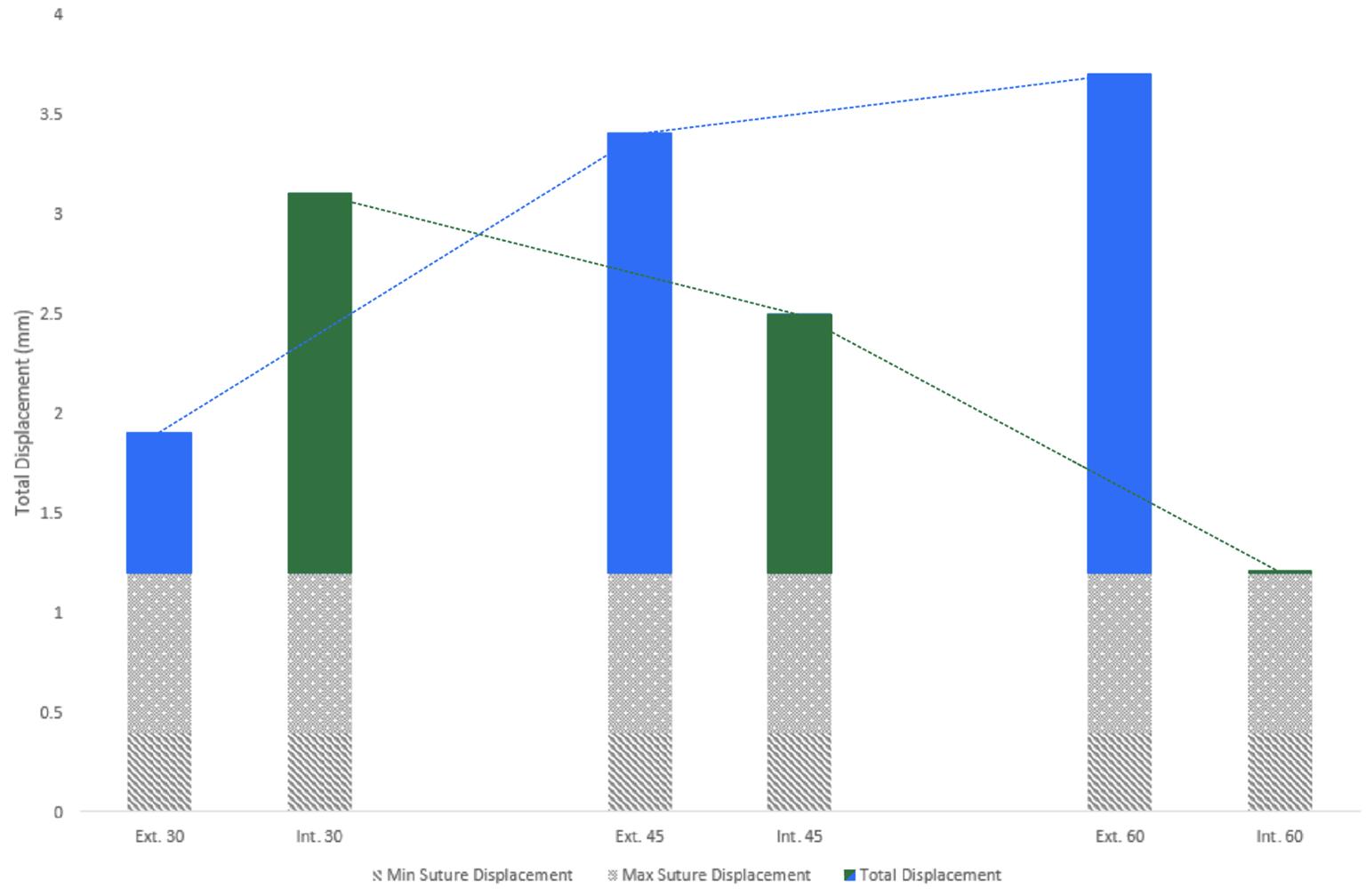
Figure 4: Contribution of Suture Elasticity to Overall Failure of External vs Internal Anchors at 30, 45, and 60 degrees
Figure 4 shows that suture anchors should be inserted into osteoporotic bone using an internal suture anchor at 60 degrees to the bone surface to reduce the combinatorial failure modes of suture elongation, anchor creep, and bone sawing. Interestingly, external anchors display increasing displacement as angle magnitude increases, whereas internal anchors display decreasing displacement with increasing angles up to a certain point.*
This graph illustrates all four of the combined failure modes of suture anchors in osteoporotic bone. This internal anchor was inserted at 90 degrees to the pull*, which is called Deadman’s angle. This data discovered novel information on the biomechanical failure modes when inserted perpendicular to the pull.
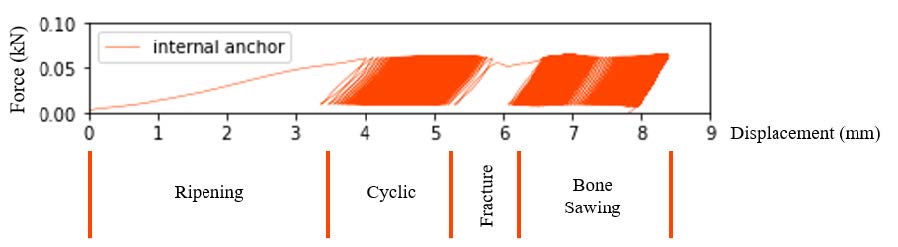
Figure 5: All Biomechanical Failure Modes of Suture Anchors in Osteoporotic Bone Displayed
V. Conclusions
By inserting an internal suture anchor at the designated “safe” angle of 60 degrees, patient suffering can be reduced. We found that the optimal angle of insertion was 60 degrees to effectively reduce the effects of suture elasticity, anchor creep, and cyclical sawing through osteoporotic bone. This finding is important because it has the potential to minimize medical costs, patient suffering, and surgical failure. With an aging population, this information is critical to better outcomes in orthopedic surgery.